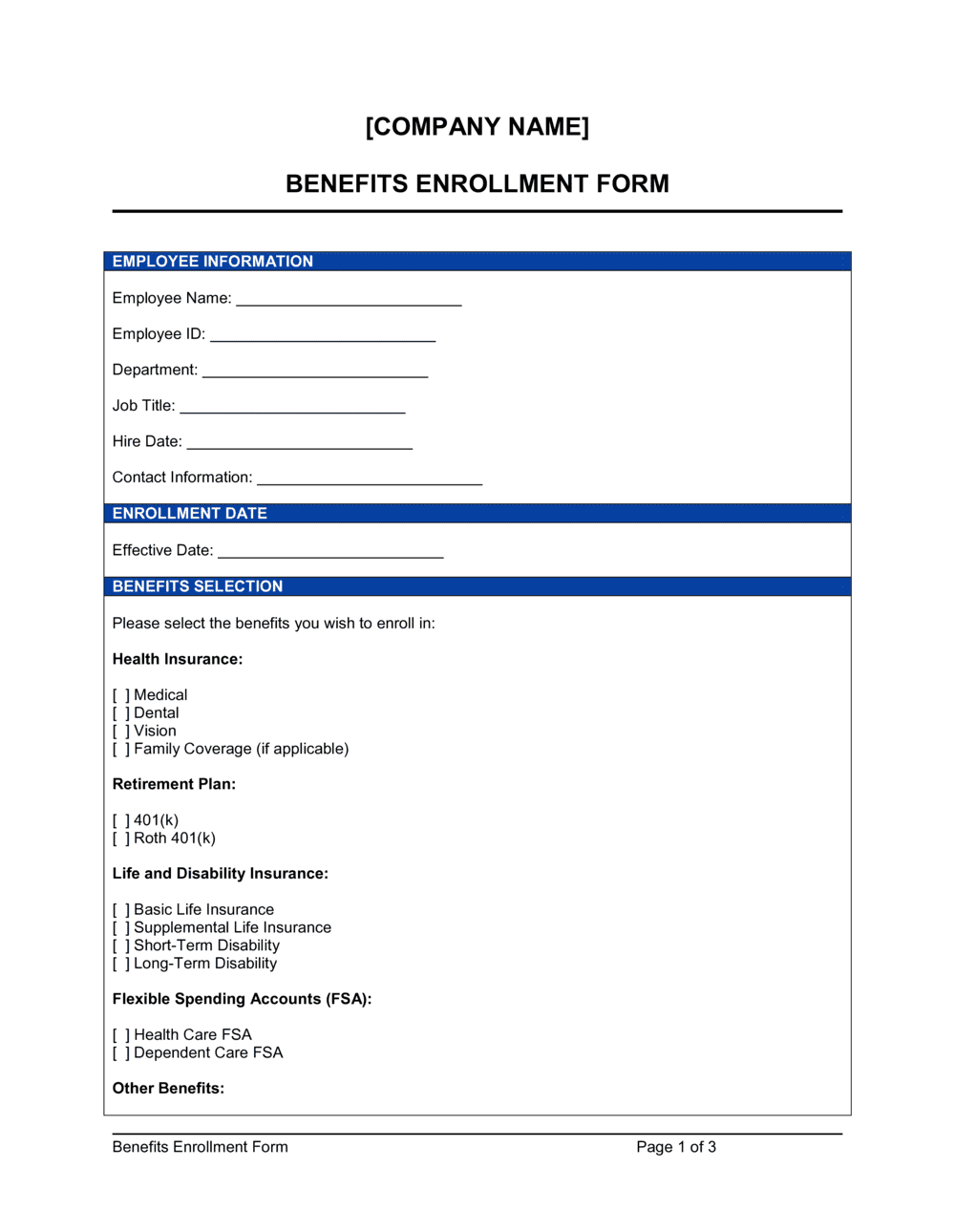
❌ Missing dependent SSNs and dates of birth
Why it matters: Carriers require date of birth and SSN to verify dependent eligibility before activating coverage. Forms submitted without this data are rejected and must be resubmitted, often missing the enrollment window.
Fix: Collect dependent SSNs and dates of birth before distributing the form so employees can complete it in one pass.